In this session, we will learn how to approach a patient with lower motor neuron weakness. When somebody presents with weakness, the lesion could be in either the upper motor neuron or lower motor neuron. Suppose the lesion is anywhere between motor cortex and spinal segmental level, including cortex, corona radiata, internal capsule, brainstem or spinal cord. In that case, the patient will be having upper motor neuron features like hypertonia, spasticity, brisk reflexes and upgoing plantar. If the lesion is in the lower motor neuron extending from the segmental anterior horn cell, root, plexus, peripheral nerve, neuromuscular junction, or muscle, there will be wasting, hypotonia, decreased reflexes, and fasciculations. We will focus on lower motor weakness in this session. We will start with a case.

Fig- 1 Upper motor neuron
A 60-year-old male patient presented with sudden onset painless buckling of the right knee on getting up in the morning. There was pain and paraesthesia in front of the right thigh and leg along with it. He has had diabetes for ten years with poorly controlled blood sugar. On examination, his higher function and cranial nerves were normal. Motor system examination showed a decreased tone of the right lower limb with grade 3 power for right knee extension and right hip flexion, adduction and abduction. Left lower limb and upper limbs were normal. His right knee jerk was asymmetrically absent. Sensory system examination showed decreased sensation in front of the right thigh and medial side of the right leg. The straight leg raising test was negative, and there was no spinal tenderness.
Now, let’s analyse this case as we learnt in episode two, Approach to weakness. When somebody presents with weakness, the first question is if it is a true weakness. A painful buckling may suggest an orthopaedic problem like osteoarthritis knee, and the patient may not have a true weakness. A painless buckling usually indicates true weakness. This patient did not have any pain in the knee but only in the front of the thigh. The presence of paraesthesia also suggests a neurological cause. Once we are sure it is a genuine weakness, the next question is if it is an upper motor neuron or lower motor neuron type of weakness. Buckling of the knee suggests quadriceps weakness which could either be due to a lower motor neuron or upper motor neuron problem. The patient had hypotonia of the right lower limb with an absent knee jerk and flexor plantar response, suggesting a lower motor neuron type of weakness. The asymmetrical decrease in knee jerk is important in these patients, indicating the lower motor neuron type lesion. Upper motor neuron lesions usually have brisk or normal reflexes except in the rare case of a spinal shock state. The site of lesion in lower motor neurone includes anterior horn cell, root, plexus, peripheral nerve, neuromuscular junction or muscle.
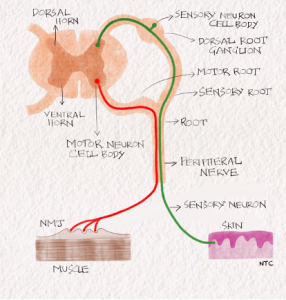
Fig -2 Lower motor neuron
Once we are sure it is a lower motor neuron problem, the next question is whether it is a pure motor or motor-sensory problem. Some components of the lower motor neuron, namely anterior horn cell, muscle and neuromuscular junction, are pure motor. The involvement of these anatomical structures will not produce any sensory symptoms. Since our patient has sensory symptoms in the form of pain and paraesthesia along with knee-buckling, we can rule out these three localisation sites in the lower motor neuron. So what is left is the root, plexus and peripheral nerve. Now let us see which of these three best fits our patient’s clinical profile.
The femoral nerve supplies the quadriceps muscle. Is it an isolated femoral nerve palsy? The buckling of the knee and paraesthesia in front of the thigh and medial side of the leg can be explained by femoral nerve palsy. The sensory on the medial side of the leg is supplied by the saphenous branch of the femoral nerve. However, the isolated femoral nerve palsy cannot explain the hip adduction and abduction weakness. The weakness is beyond the femoral nerve, and the obturator nerve and superior gluteal nerve are also involved. Multiple nerves in a single limb are involved, which usually occurs with a plexus lesion. The immediate differential diagnosis will be multiple roots involvement, namely L2, L3, L4 and L5 roots on the right side. The foot dorsiflexion and hip abduction are both supplied by the L5 root. Suppose the hip abduction weakness was due to L5 root we except the foot dorsiflexion also to be weak. The severe pain at the onset of symptoms which is not radicular, make right lumbosacral plexopathy the first possibility. Poorly controlled diabetic patients are prone to diabetic lumbosacral plexopathy, otherwise known as diabetic amyotrophy. Early diagnosis is critical in these patients as quadriceps wasting occurs fast in these cases as in other plexopathies. The immediate differential diagnosis will be L2, L3, L4 root lesion on the right side. Imaging the Lumbosacral spine and plexus, nerve conduction study and electromyography of the involved muscles should confirm our diagnosis.
The patient had an HBA1C of 13. MRI lumbosacral spine did not show any lesion involving right L2, L3, L4 root. MRI lumbosacral plexus showed enhancement of the upper lumbosacral plexus consistent with the clinical diagnosis of plexopathy. There was no infiltrative or compressive lesion. NCS and EMG were also consistent with the clinical diagnosis of lumbosacral plexopathy. The patient was treated with pulse methylprednisolone along with strict glycaemic control and physiotherapy. The patient recovered completely at one month follow up.
This case highlights the importance of early diagnosis in lower motor neuron disease. Any delay in diagnosis will result in the early development of muscle atrophy and permanent disability. It again illustrates the ease with which we can come to a provisional diagnosis when we have a clinical approach.
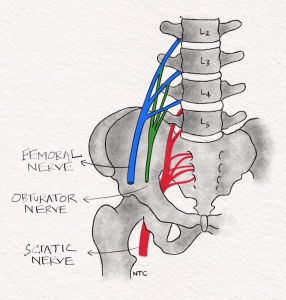
FIG-3 Femoral nerve arising from L2, L3, L4 roots and lumbosacral plexus.
Now let us see the clinical features of individual Lower motor neuron components. First, we will see the pure motor components, which includes anterior horn cell, muscle and neuromuscular junction disorders. It’s important to note that a motor-sensory component can also present as a pure motor syndrome if the sensory is not involved. For example, a disc compressing only to the ventral motor root can produce a pure motor syndrome, though the lesion is at the root level, which usually causes a sensory-motor syndrome. Similarly, lead palsy has a preference for peripheral motor nerves. It can also produce a pure motor syndrome though the affection is in peripheral nerves, which usually make a sensory-motor syndrome.
Muscle
First, we will see the clinical features of muscle disease. We will start with a case. A 60-year-old female presented with difficulty in getting up from squatting of 4 months duration. For the last three months, she has been having buckling of both knees and difficulty raising the arm above the shoulder. There was no distal weakness or sensory symptoms. On examination, she had a waddling gait. There was Grade 3 proximal upper limb and lower limb power with normal tone and reflexes. Her CPK was 10000, electromyography showed a myopathic pattern, and muscle biopsy showed inflammatory myopathy- polymyositis. She was treated with immunosuppressants with symptomatic improvement.
This case is a prototype myopathy, and the clinical features include
Pure motor syndrome
Proximal and symmetrical weakness
No significant wasting or fasciculation.
Reflexes are usually retained until the late stages.
EOM and bulbar muscles can be variably involved in different types of muscle disease and help to differentiate between them.
There is no fatiguability or diurnal variation of symptoms which are features of NMJ disorders.
Exemptions to the usual clinical pattern can occur. It can be asymmetrical as in FSHD or inclusion body myositis. It can be distal predominant as in myotonic dystrophy or other distal myopathies.
CPK elevated in most but not all cases.
Remember that muscle disease produces a pure motor symmetrical proximal weakness without fatiguability or diurnal variation.
Neuromuscular junction disorders
Once again, we will start with a case to have a mental picture of the patient’s symptoms. A 30-year-old female presented with diplopia and drooping of the eyelid of 3 months duration. The drooping was more towards evening. She had difficulty chewing and swallowing for the last two months. The symptoms were mild when she started eating and increased as she continued. For the previous month, she had a nasal twang of voice and difficulty in climbing stairs. On examination, she had bilateral ptosis with weakness of EOM, which was not in a nerve distribution. Pupils were normal. She had weakness of eye closure and neck extensors causing her head to drop while sitting. Her tone and reflex were normal. There was grade 4- power in proximal upper and lower limb with demonstrable fatiguability. Sensory examination was normal. Ice pack test and neostigmine test was positive. RNS at 3Hz showed a decremental pattern suggestive of postsynaptic neuromuscular junction disorder. The acetylcholine receptor antibody was positive confirming the clinical diagnosis of myasthenia gravis. The patient responded well to pyridostigmine and steroids, followed by immunosuppressants. Myasthenia gravis is the prototype NMJ disorder. The clinical features include
Pure motor syndrome
Proximal and symmetrical weakness
Early ptosis and EOM involvement
Bulbar involvement
Fatiguability and Diurnal variation are the most characteristic features.
Reflex normal mostly except in LEMS
Remember that NMJ disorders like myasthenia produce pure motor proximal symmetrical weakness with early EOM and bulbar involvement. Fatiguability and diurnal variation are the characteristic findings that differentiate them from muscle disease.
Anterior horn cell disease
A 45-year-old male patient presented with wasting and weakness of the right upper limb of 3 months duration. On examination, he had weakness and wasting of the deltoid, biceps, and small hand muscles on the right side. There was mild weakness of the left upper limb and both lower limbs as well. The Biceps reflex was exaggerated in the weak and wasted right side. The lower limb reflexes were brisk, and the plantar was extensor bilaterally. The patient had extensive fasciculations all over the body, including the tongue. Sensory examination was normal. MRI brain and spine were normal. Nerve conduction study and electromyography were consistent with the clinical diagnosis of motor neuron disease -ALS. ALS is the prototype anterior horn cell disease. The clinical features of motor neuron disease include
Pure motor syndrome
Either UMN alone as in primary lateral sclerosis or LMN alone as in SMA. ALS is the only motor neuron disease where both upper and lower motor neuron is involved.
Asymmetrical mostly
Prominent wasting and fasciculations.
It may be acute as in polio or chronic as in ALS
LMN and UMN findings in ALS
EOM not usually involved
No bowel and bladder involvement.
Motor sensory syndromes
Now, let us focus on the sensory-motor syndromes of LMN. It includes peripheral nerve, plexus and root involvement.
Peripheral nerves
Peripheral nerves can present in three ways. This includes
1. Mononeuropathy as in carpal tunnel syndrome where motor and sensory impaired in the distribution of a single nerve
2. Mononeuritis multiplex
Multiple peripheral nerves are involved at different locations.
For example, right radial nerve and left CPN.
Motor and sensory impairment in the distribution of these nerves
Hansen disease and vasculitis are the common causes
3. Peripheral neuropathy
Peripheral nerves are involved in a length-dependent manner.
Distal stocking and glove sensory loss
Symptoms start in the foot and slowly ascend to the knee. By the time it reaches the knee, the symptoms appear in the hands in a length-dependent manner.
First motor symptoms are usually slipping of chappals with or without knowledge.
The toe grip will be weak.
Dorsiflexion more week than plantar flexion
Diabetic peripheral neuropathy is a classic example.
Plexus
We already discussed a case of diabetic lumbosacral plexopathy in the beginning. Let’s revise the clinical features.
Multiple peripheral nerves in a single limb affected
Usually asymmetrical and one limb alone is affected.
Rarely bilateral amyotrophy can occur in diabetes.
Severe pain at onset and early wasting are other characteristics of plexopathy.
Examples are Parsonage turner or idiopathic brachial plexitis and diabetic amyotrophy.
Root
The clinical features of root involvement include
Radicular pain – pain in the distribution of dermatome which increases on coughing and straining
There is weakness in the distribution of muscles supplied by the root.
Sensory loss in a dermatome may not be appreciated when a single root alone is affected due to the overlap of adjacent dermatomes.
Three types of involvement
1. Single root as in disc prolapse. C5 Root involvement due to cervical disc prolapse compressing on to exiting root. The patient will have decreased biceps and supinator jerk with radicular pain in the C5 dermatome. Weakness may be present in C5 innervated muscles.
2. Multiple roots as in Cauda equina. Multiple roots are involved in the spinal canal below L1 vertebrae due to disc prolapse or tumour. Usually asymmetric as the roots are variably involved on either side.
3. Polyradiculopathy as in GBS. Multiple roots and nerves are affected all over the body. The patient will have generalised areflexia with an ascending motor sensory syndrome. The weakness is proximal more than distal usually. Bilateral facial nerve involvement and absence of bowel and bladder involvement helps to differentiate from acute myelopathy in a spinal shock state.
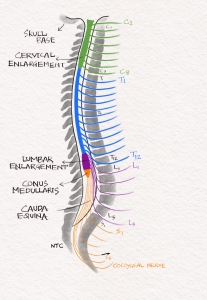
FIG-4 Cauda equina is the collection of roots in the spinal canal below L1 vertebra. The spinal cord ends as conus medullaris at L1 vertebral level.
We have finished the clinical features of all the components of LMN. Let’s revise the steps to approach a case of weakness once again.
Step 1: Is there a true weakness?
Step 2: If yes, is it upper motor neuron or lower motor neuron?
Step 3: If lower motor neuron, is it pure motor or motor-sensory?
Step 4- If pure motor syndrome, Anterior horn cell, muscle or neuromuscular junction disorder based on further clinical findings. Asymmetrical weakness with wasting and fasciculation suggest anterior horn cell. Symmetrical proximal weakness with early EOM involvement with fatiguability and fluctuation suggest neuromuscular junction disease. Pure motor proximal weakness without fatiguability and fluctuation suggest muscle disease.
Step 5: If motor-sensory syndrome, root, plexus or peripheral nerves, based on the distribution of motor weakness and sensory loss.
We will solve one last case using these steps before wrapping up.
A 28-year-old male presented with paraesthesia of both lower limb of 4 days duration and weakness of lower limb followed by the upper limb of 3 days duration. No bowel and bladder involvement. On examination, he had a bifacial weakness. He had hypotonia with generalised areflexia. His plantar was flexor. He had grade 2 power in proximal upper and lower limbs with grade 4 power distally and needed walking support. JPS was impaired in both upper and lower limbs. There were no cerebellar signs. The autonomic nervous system, skull and spine were normal. Let’s approach this case now.
Step 1: Is there a true weakness?
Yes, he does have a true weakness.
Step 2: If yes, is it upper motor neuron or lower motor neuron?
Since the patient has hypotonia with areflexia and no bowel and bladder involvement, this is more likely to be LMN.
Step 3: If lower motor neuron, is it pure motor or motor-sensory?
It is a motor-sensory syndrome. So the possibilities are root, plexus and peripheral nerve. Plexus is unlikely as all four limbs are affected. What is left is the root and peripheral nerve. This disease is a polyradiculoneuropathy where multiple roots and peripheral nerves are affected. It is caused by an acquired demyelinating disease called GBS. So final diagnosis for the patient is
Functional deficit- Areflexic quadriparesis with bifacial weakness
Anatomical localisation- Motor sensory lower motor neuron syndrome with multiple roots and nerve involvement
Aetiology- GBS
NCS showed an acquired demyelinating polyneuropathy. CSF showed albumin-cytological dissociation consistent with the clinical and electrophysiological diagnosis of the AIDP subtype of GBS. The patient was treated with plasma exchange followed by physiotherapy with complete resolution of symptoms.
That finishes today’s discussion. Thank you all for the tremendous support we have been receiving from around the world for our podcast. Please go through the notes and images of this discussion at the neurologyteachingclub.com website. The link to the website is in the show description. Please enrol for the newsletter at the website. Then the new episodes will reach directly to your mailbox along with other goodies. If you hear this on an Apple device, please give a rating and leave a review. You can do this by touching on the three dots on the top left corner of the screen and then clicking on, go to show and scrolling down. I am telling apple specifically because that is the only platform that provides this feature currently. Your review will be a huge encouragement for us to continue working hard to bring the show to you. If you liked the podcast, please share it with your friends and colleagues. If you have some comments and suggestions, let us know at the comment box on the website. We will love to hear from you.