Ataxia is a common symptom with which a patient presents to a neurologist. An ataxia case is often kept for final year medical school clinical examination. Ataxia is defined as a lack of voluntary coordination of muscle activity. A cerebellar pathology usually causes ataxia, but it can be caused by defects in proprioception and vestibular function. The cerebellum regulates muscle tone, posture, and equilibrium. One of the major cerebellar functions is the automatic excitation of the antagonist muscles at the end of a movement, with the simultaneous inhibition of agonist muscles that initiated the movement. The cerebellum acts as the orchestra’s conductor and finely coordinate the gross movements done by the pyramidal system. Cerebellar ataxia results from defective timing of the sequential contraction of the agonist and antagonist. The movements err in speed, range, force and timing. A patient with sensory ataxia will have sensory symptoms like paresthesia, and ataxia will be more on closing eyes, usually described as a washbasin sign. Patients with vestibular ataxia often have vertigo. Both vestibular and sensory ataxia won’t have other features of cerebellar ataxia like dysarthria, tremor etc. We will focus on cerebellar ataxia in this session. We will learn the approach to a patient with cerebellar ataxia. At the end of the episode, we will understand
-
- The cerebellar anatomy and connections of the cerebellum.
- The symptoms produced by lesions of the cerebellum.
- Localise from symptomatology of the patient, which part of the cerebellum is involved.

Fig -1 Midsagittal section of the cerebellum.
The cerebellum is located in the posterior fossa. It lies dorsal to the pons and medulla oblongata. It is separated from the occipital lobes by the tentorium cerebelli. It has a midline portion, the vermis, and two lateral portions, the cerebellar hemispheres. It has two fissures which divide it into three lobes. The primary fissure divides it into anterior and posterior lobes. The posterolateral fissure separates the posterior lobe from the flocullonodular lobes. From an embryogenetic and functional standpoint, the cerebellum can be divided into
1. The archicerebellum.
2. The paleocerebellum.
3. The neocerebellum.
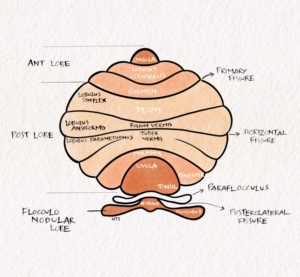
Fig -2 Schematic diagram of cerebellum showing lobes and lobules.
The archicerebellum corresponds to the flocculonodular lobe. It is otherwise called the vestibulocerebellum because it has several connections with the vestibular nucleus. It also receives input from areas concerned with eye movements. As a result of these connections, the archicerebellum controls body equilibrium and eye movements.
The paleocerebellum consists of mainly the vermis of the anterior lobe. It is also known as the spinocerebellum because it receives input primarily from the spinal cord. It plays a role in controlling muscle tone and axial and limb movements.
The neocerebellum consists of most of the cerebellar hemispheres. Since it receives projections from the pons through the corticopontocerebellar pathway, it is also termed the pontocerebellum. The neocerebellum projects fibres to the cerebral cortex through the thalamus and plays a role in planning, initiating, and regulating fine limb movements.
The cerebellum has 85 billion neurons. The cerebellum consists of a superficial cortex surrounding the deep white matter. Three pairs of nuclei lie in the deep white matter. The cortex of the cerebellum is folded into the cerebellar folia.
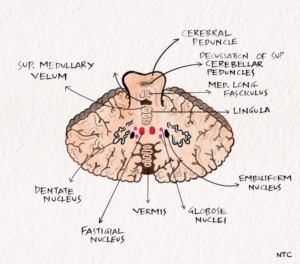
Fig –3 Axial section of cerebellum showing the deep nuclei.
Cerebellar nuclei
The cerebellar nuclei are the main source of cerebellar efferents. All of the efferent projections of the deep cerebellar nuclei are excitatory, except for projections to the inferior olive, which are inhibitory. These nuclei from medial to lateral include the fastigial nucleus, the nucleus interpositus (composed of the globose and emboliform nuclei), and the dentate nucleus. The arrangement can be remembered by the code Fast Girls Eat Dates.
The fastigial nucleus assists stance and gait. Therefore its lesion may cause abasia. You can remember it by the code- Fast Gait.
The nucleus interpositus assists segmental reflexes. It speeds the initiation of movements triggered by somatosensory cues. It guides the response, stop unwanted and promotes wanted oscillations. Therefore, nucleus- interpositus lesions may result in delayed check or rebound responses, truncal titubation, abnormal rapid alternating movements, action tremor, and ataxia on finger-nose-finger and heel-knee-shin manoeuvres.
The dentate nucleus assists in tasks requiring fine dexterity. You can remember it like D for D [Dentate for Dexterity]. Lesions of this nucleus or its projections cause delays in initiating and terminating movements, terminal and intention tremors, temporal incoordination in activities that require multiple joints, and abnormalities in the spatial coordination of hand and finger movements.
The cerebellar peduncles.
The cerebellum is connected to the brainstem through the superior, middle and inferior cerebellar peduncle. The superior mainly contains outgoing tracts, while the middle and inferior mostly have incoming tracts. The superior cerebellar contains mainly efferents to the red nucleus and thalamus, namely dentatorubral and dendatothalamic tract. The middle cerebellar peduncle contains mainly afferents from contralateral pontine nuclei, namely the pontocerebellar or corticopontocerebellar tract. The inferior cerebellar peduncle contains mainly afferents from the spinal cord and brainstem. These include spinocerebellar, olivocerebellar and vestibulocerebellar. The peduncles have a few other afferent and efferent tracts.
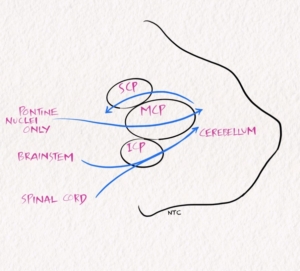
Fig- 4 Afferent and efferent tracts in cerebellar peduncle.
Clinical features of the cerebellar disease include
-
- Ataxia
- Dysarthria
- Tremor
- Hypotonia
- Eye movement abnormalities
- Non motor manifestations
Ataxia
Ataxia is caused by the defective timing of sequential contraction of agonist and antagonist. The movements err in speed, range, force and timing. The components of ataxia include
1. Asynergia- lack of synergy of various muscle components.
2. Dysmetria – abnormal range, force, and excursion in movement.
3. Dysdiadokokinesia- impaired rapidly alternating movements.
4. Rebound phenomenon- when an opposed motion is suddenly released, an impaired checking response and excess rebound.
Gait ataxia
A patient with cerebellar gait ataxia has a wide-based gait. They can fall in any direction. Trunkal ataxia and titubation suggest midline cerebellar lesion.
Cerebellar dysarthria
There is an abnormality in articulation and prosody in patients with cerebellar disease. There is laboured speech production with occasional facial grimacing. They will have a scanning speech. It is more common with hemisphere involvement. Agrammatism is noticed with the right cerebellar lesion and aprosody with the left. The cerebral connections of the cerebellum are predominantly contralateral accounts for this.
Tremors
Tremors occur with lesions affecting the dentate nucleus. Kinetic or intention tremors occur during activity. A static postural tremor may also occur due to interruption of the rubro-olivo-cerebellar circuit. Cerebellar fits are episodes of decerebrate rigidity usually seen in large midline cerebellar mass lesions.
Hypotonia
Hypotonia occurs in hemispheric lesions acutely. It is ipsilateral and more in proximal upper limbs, though pendular jerk is demonstrated in the knee. It is due to decreased fusimotor activity due to injury to the dentate nucleus resulting in reduced response to stretch in muscle spindle afferents.
Oculomotor dysfunction
A wide range of eye movement abnormalities can occur with cerebellar lesions. We will see what they are but won’t go to the details.
In midline cerebellar lesion
1. Gaze evoked nystagmus
2. Upbeat nystagmus
3. Rebound nystagmus
4. Abnormal optokinetic nystagmus
Lesions of the uvula and nodulus produce periodic alternating nystagmus.
Lesion of the vestibulocerebellum and posterior midline causes down beating nystagmus.
Other ocular signs include
Broken pursuit
Ocular flutter
Opsoclonus
Ocular bobbing
Paresis of conjugate gaze
Skew deviation
Square wave jerk at rest
Ocular tilt reaction
Failure to suppress the vestibulo-ocular reflex.
Non-motor functions of the cerebellum.
There is growing evidence that the cerebellum plays a role in cognition. Acute pan cerebellar involvement are more commonly associated with cognitive dysfunction, which includes
Impaired executive dysfunction
Personality change
Disinhibition
Language dysfunction including agrammatism, aprosody
Visuo spatial memory impairment
Pathological laughter due to the corticoponto cerebellar fibre involvement and macrographia.
The disruption of cerebellar modulation of neural circuits linking prefrontal, post parietal, superior temporal, limbic cortices is implicated in cognitive dysfunction. Cerebellar dysfunction plays a role in the pathophysiology of schizophrenia, bipolar disorder, addiction, autism and dyslexia.
Clinical syndromes of the cerebellum
- Cerebellar pathology produces four clinical syndromes based on the areas of cerebellar involvement.
- The rostral vermis syndrome with lesions of the anterior lobe
- The caudal vermis syndrome with lesions of the flocculonodular and posterior lobe
- The hemispheric syndrome with lesions of the posterior lobe and variably the anterior lobe
- The pan cerebellar syndrome
Rostral vermis syndrome
The anterior and superior vermis is predominantly involved in rostral vermis syndrome. Gait ataxia is the most prominent symptom. The patient will have a wide-based stance. Limb incoordination, dysarthria, hypotonia and nystagmus are not apparent. The classic example is alcohol-induced cerebellar dysfunction.
Caudal vermis syndrome
There is damage to the flocculonodular lobe. The patient will have axial disequilibrium and a staggering gait. Spontaneous nystagmus and rotated head posture are common. There is no limb ataxia. The caudal vermis syndrome is classically seen in medulloblastoma in children.
Cerebellar hemispheric syndrome
There is damage to the cerebellar hemisphere on one side. The ipsilateral appendicular movements are affected. The patient will have abnormal finger-nose finger, heel knee shin and dysdiadokokinesia on the same side. Dysarthria is often present. Infarcts, neoplasm, abscesses etc., cause the hemispheric cerebellar syndrome.
Pan cerebellar syndrome
The whole cerebellum is involved, and a combination of all previous symptoms are seen. The patient will have bilateral cerebellar signs. The etiologies include drugs and toxins, infectious and post-infectious like following chickenpox. Metabolic causes like hypothyroidism and Paraneoplastic like anti hu in small cell ca lung, anti yo in breast carcinoma, anti tr in lymphoma also produce a pan cerebellar syndrome.
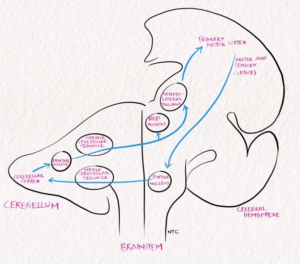
Fig- 5 Frontopontocerebellar and dentatorubrothalamocortical pathways.
Before we wind up, let us learn one more syndrome we commonly come across in the clinics, ataxic hemiparesis. It is not a cerebellar syndrome but due to a lesion in the cerebellar connection, namely the frontopontocerebellar fibres. The patient will have mild pyramidal weakness along with ataxia. It is one of the lacunar syndromes due to a small infarct in the pathway of frontopontocerebellar fibres. The usual site is the basis pontis at the upper one-third and lower two-thirds junction. The weakness and ataxia are more prominent in the opposite lower limb. Dysarthria and nystagmus may be present. There is hyperreflexia, and the Babinski sign is usually positive. This syndrome is also described with lesions in the opposite side thalamocapsular region, posterior limb of the internal capsule, red nucleus, and paracentral area. These patients are often mistaken as having hemiparesis alone. The disproportionate functional deficit in the presence of mild weakness is the clue, and examination will show the cerebellar signs.
That finishes this session. Today we discussed the various causes of ataxia. We discussed cerebellar ataxia in detail, along with the cerebellar anatomy and its connections. We discussed the clinical features of cerebellar disease and the various clinical syndromes. In the next session, we will discuss the brainstem.
It’s been more than six months since we started our podcast. Thank you all for the tremendous response from all over the world. The podcast has been downloaded more than 8000 times from our 80 countries. Please continue your valuable support and share with your friends and colleagues if you find the podcast useful. Kindly write a review and give a rating in the Apple podcast. Spotify has started rating for podcasts. The ratings will help to increase the visibility of the podcast in the app. Please provide your feedback and suggestions on the website or Twitter. It will be a big help and will be much appreciated.