Hello everyone, This is a bonus episode of the blood supply of the brain. Episode 7 was almost reaching twenty minutes. I could not give a summary in the episode, and many of you were asking about the blood supply of the internal capsule, which is a standard short note for exams. I thought I would make a short bonus episode to give a summary of the last episode and discuss the blood supply of the internal capsule. For the full discussion, please hear episode 7, the blood supply of the brain and arterial localisation of stroke.
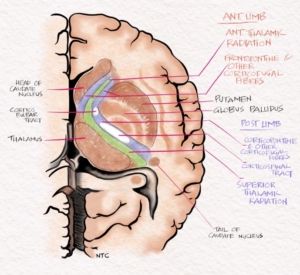
Fig -1 Coronal section of brain through the internal capsule.
The Internal carotid artery terminates as the Middle cerebral artery and Anterior cerebral artery. The Anterior cerebral artery supplies the medial surface of the brain. The Anterior cerebral artery is divided into proximal A1 and distal A2 segments by the Anterior communicating artery. The occlusion of A1 will not produce much of symptoms since the A2 will get blood from the opposite side through the Anterior communicating artery, and there is a rich anastomosis around the Circle of Willis. A2 proximal occlusion produces opposite lower limb weakness and urinary incontinence as the leg area of the motor cortex and paracentral lobule lies in the medial surface of the brain supplied by the anterior cerebral artery. There will be some frontal lobe dysfunction like apathy. The Recurrent artery of Heubner is a penetrating branch of ACA arising from the A1-A2 junction or proximal A2. It supplies parts of the internal capsule and caudate nucleus. The occlusion of the Recurrent artery of Heubner produces opposite site faciobrachial monoparesis due to the internal capsule involvement. The occlusion of the A2 proximal to the origin of the Recurrent artery of Heubner will result in opposite side hemiparesis with urinary incontinence. An unpaired anterior cerebral artery is a congenital anomaly where one side A1 is absent from birth and a single A1 supply both A2 through the Anterior communicating artery. The occlusion of an unpaired Anterior cerebral artery will result in acute paraplegia as both sides leg areas are affected.
The middle cerebral artery supplies 2/3 of the brain. The part of the middle cerebral artery before the bifurcation is called M1. The occlusion of proximal M1 results in a massive stroke with hemiplegia, hemianopia and hemianesthesia of the opposite side. In left-sided occlusion, the patient will have cortical features in the form of global aphasia and right-sided occlusion neglect. The patient’s sensorium is usually poor due to brain oedema, and they are at high risk for herniation and death. The lenticulostriate arteries are the penetrating branches of the middle cerebral artery, and they supply the capsuloganglionic area. Infarct in these small arteries produces the classic lacunar syndromes: hemiparesis, hemianesthesia, ataxic hemiparesis, and dysarthria clumsy hand syndrome. The middle cerebral artery divides into a superior and inferior division. The superior division occlusion on the dominant hemisphere produces right hemiparesis with Broca’s aphasia. The inferior division occlusion causes Wernicke’s aphasia with superior quadrantanopia.
The posterior cerebral artery supplies manly the occipital lobe. The P1 lies proximal to the posterior communicating artery and P2 distal to it. The penetrating branches of P1 supply the thalamus and midbrain. Occlusion causes hemianesthesia and the classical midbrain syndromes like Weber and Benedict. The P2 occlusion produces a macula sparing homonymous hemianopia of the opposite side. The proximal P1 occlusion has a combination of the above symptoms.
The Internal carotid artery occlusion produces similar symptoms to the middle cerebral artery infarct. The involvement of the Ophthalmic artery is the clue to differentiate an Internal carotid artery occlusion from the middle cerebral artery. The anterior choroidal artery is another direct branch of the Internal carotid artery. The occlusion produces a combination of hemianesthesia, hemiplegia and hemianopia of the opposite side of the body. The lesion is in the internal capsule so that the patient won’t have any cortical features.
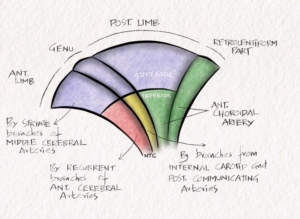
Fig 2- Schematic diagram showing blood supply of the Internal capsule.
The blood supply of the internal capsule
The blood supply of the internal capsule is variable. The superior part of the anterior limb, Genu and posterior limb are supplied by lenticulostriate branches of the middle cerebral artery. The recurrent artery of Heubner supplies the inferior aspect of the anterior limb. The inferior part of Genu is supplied by direct branches from the internal carotid artery and posterior communicating artery. The anterior choroidal artery supplies the inferior part of the posterior limb of the internal capsule. The retrolentiform and sublentiform parts of the internal capsule are supplied by the anterior choroidal artery and the branches of the posterior cerebral artery. Please see and learn the schematic diagram on our website neurologyteachingclub.com or Instagram page to remember this easily.
That’s it for now. I hope you enjoyed the bonus episode. Please leave your commands, suggestions and opinion on our website. The link is given in the show notes. Last month Dr Anu from the UK gave some valuable suggestions, which I have incorporated in this episode. Thank you, Dr Anu and looking forward to more such feedback from all of you.